Why is the surface of an implant so important?
In biomaterials engineering, it’s easy to fall back on the intuition derived from traditional materials science: since an implant must withstand loads, not corrode, not wear down excessively, and function for years, its success should depend primarily on the material “inside.” This is only part of the truth. The bulk material is indeed responsible for strength, stiffness, elasticity, durability, and permeability. However, from the body’s perspective, the first and most important contact occurs not with the entire block of material, but with its outer layer. It is this layer that comes into contact with blood, proteins, cells, and bodily fluids. In practice, this means that an implant can be mechanically very good yet biologically problematic if its surface sends the “wrong signal” to the tissues.
This observation changes the way we think about implant design. Instead of asking only “what should the implant be made of?”, we must consider what the implant’s surface should be like. In biomaterials, the biological response is not a simple reflection of the chemical composition of the entire component. Rather, it is a response to what happens at the material–tissue interface: the surface chemistry, wettability, charge, roughness, organization, and reactivity. This is why the success of an implant is so often determined not by the volume of the material, but precisely at the phase boundary.
This article is based on Biomaterials Science: An Introduction to Materials in Medicine, ed. William R. Wagner et al., 4th ed., 2020. The following content is only a general overview of the topic. For those interested in the subject, we recommend delving into the literature.
How does the body react to the surface of a material?
The most important starting point is simple: the body does not “see” the entire implant at once. First, it “reads” its surface. The authors of Biomaterials Science state explicitly that for materials that do not release undesirable substances, the transfer of information from the material to proteins, cells, and the entire body occurs through the surface structure. The body, therefore, responds to the specific chemistry and organization of the outer layer, rather than to the averaged properties of the entire material. This seemingly minor shift in emphasis has enormous practical significance, as it moves the issue of biocompatibility from the level of “what kind of alloy or polymer we have” to the level of “how its interface looks and behaves.”
It is important to remember that the surface is not simply a thin end of the material that behaves the same as its interior. The book emphasizes that the surface is a zone of particular reactivity and almost inevitably differs from the bulk. For a real metallic material, the outer layer may include not only metal oxide but also adsorbed water, polar organic compounds, and hydrocarbon contaminants. For polymers, the unique surface zone can range from about 10 to 100 nm. This is important because it means that even if the bulk material is homogeneous, its biologically active portion can be chemically and structurally complex.
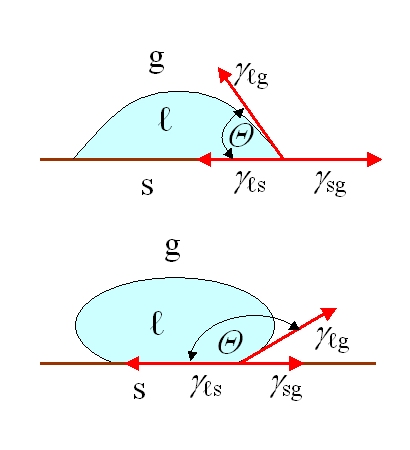
From a biological perspective, the surface is not merely a matter of chemical composition. The authors list many features that can influence biological responses: roughness, patterns and topography, wettability, surface mobility, chemical composition, electrical charge, crystallinity, elastic modulus, and heterogeneity. At the same time, they honestly note that it is not yet possible to identify a single universal feature that is most important for every biological response. In practice, this is a very engineering-oriented lesson; one must not base a design on a single parametric slogan such as “let’s increase roughness” or “let’s make the surface more hydrophilic,” because the body’s response is the result of the interaction of several characteristics at once.
This approach explains why two implants made from the same bulk material can behave biologically differently. A change in processing, sterilization, storage, or packaging is enough to alter the surface condition. The book even highlights such mundane issues as fingerprints, additives migrating from packaging, or contaminants from paper or film. In the lab, this is a detail, but in reality, it is precisely such details that can cause us to test a surface that is not the one actually present on the implant used clinically.
How the surface translates to biocompatibility
If the surface is the primary language of communication between the implant and the body, we must ask what this dialogue looks like. One of the key mechanisms is protein adsorption. The source emphasizes that after implantation of a synthetic biomaterial, adhesive proteins adsorb onto its surface very quickly, within seconds. In this way, a material that in itself lacks biological recognition motifs becomes “readable” to the body. In other words, cells often do not react directly to the pure material, but to the layer of proteins that forms on its surface shortly after contact with the body.
This has a fundamental implication for understanding biocompatibility. Biocompatibility does not merely mean the absence of acute toxicity. It signifies the material’s ability to elicit an appropriate host response in a specific application. This “appropriate response” may mean one thing for a stent, another for an orthopedic implant, and yet another for a catheter. In each of these cases, the surface controls the initial biological events: which proteins will adsorb, in what configuration, which cell receptors will be stimulated, and whether the signal will proceed toward tissue integration, platelet activation, biofilm formation, or a foreign body reaction.
A good example is the comparison of adhesion proteins and passivation proteins. The book describes how pre-coating a surface with fibronectin increases the adhesion of many cells, while albumin can limit it. This is not just a curiosity from cell culture, but a model of what happens on implants. The surface is not a neutral backdrop. It sets the initial conditions for the subsequent cellular response. In practice, this means that two surfaces with similar mechanical strength can lead to completely different healing trajectories simply because they establish the first layer of adsorbed proteins differently.
Equally important are the interactions between the surface and microorganisms. In the chapter on biofilms, the authors note that wettability, charge, roughness, and topography influence bacterial adhesion. The general trend is that greater roughness often promotes bacterial adhesion, and hydrophobic surfaces more frequently facilitate bacterial attachment. At the same time, this is not a rule without exceptions, as extremely superhydrophilic or superhydrophobic systems may act as biofilm inhibitors through a different mechanism. In practice, this serves as a cautionary note: a solution beneficial for tissue integration will not always be equally beneficial for controlling bacterial colonization.
Below is an English-language video titled BIOE 5820 Biomaterials Protein Adsorption, which is a lecture on protein adsorption on biomaterial surfaces.
Why modify the surface rather than the entire material
This is the main rationale behind surface modification. If the bulk material is responsible for load-bearing capacity, durability, and mechanical function, while the surface is responsible for biointeraction, it makes the most sense to preserve what works well in the bulk and modify only what comes into contact with the tissue. This is precisely how the authors of the chapter on physicochemical surface modifications put it: the goal is to preserve the key physical properties of the biomaterial while altering only the outer layer to improve or modulate the biological response at the tissue–device interface.
This approach has several very practical advantages. First, there is no need to abandon a material that is well understood mechanically and technologically. Titanium, steel, engineering polymers, or elastomers can continue to fulfill their structural or functional role. Second, the biological response can be more precisely tailored to a given application. We want a different surface for a bone implant, a different one for a component in contact with blood, and yet another for a catheter, where the priority may be to limit protein adsorption and the adhesion of cells or bacteria. Third, surface modification allows for improving a device without having to completely redesign the entire structure. The book even emphasizes that for devices already well-established in clinical practice, this is a way to alter biointeractions without redesigning the product, retooling production, or retraining medical staff to use the new solution.
There is, however, a condition: one must distinguish between a real modification of the interface and a cosmetic change in the description. The mere declaration that a material is “bioactive” or “antifouling” means little if it is unknown what the actual surface looks like in its final form after processing and sterilization. The source notes that the analyzed sample should correspond as closely as possible to the material or device in the form used for biological testing or implantation. This is important because the surface exposed to air may not be the same surface that the material exhibits in the body’s aqueous environment.
Three main methods of surface modification
The first method involves altering the existing surface without adding a separate, new layer. Atoms, molecules, and bonds already present in the material’s outer layer can be chemically or physically transformed. This group includes, among others, etching, chemical activation, mechanical roughening, ion implantation, and certain laser treatments. The point is that we do not “attach” a new layer to the implant, but rather remodel its own surface. This is advantageous where strong integration of the modification with the substrate is important, as well as reducing the risk of delamination and altering properties such as reactivity, wettability, corrosion resistance, hardness, or bioactivity. The source shows, for example, that ion implantation can improve wear resistance or corrosion resistance, and laser processing can controllably alter surface roughness, crystallinity, and chemistry.
The second approach involves applying a new layer or coating. In this case, a material with a different composition or properties is placed on the existing surface. This can be a thin film, a grafted layer, a polymer coating, or a system designed as a non-fouling surface. This strategy is particularly valuable when the substrate has ideal mechanical properties but is too “raw” from a biological standpoint. A good example is surfaces resistant to nonspecific protein adsorption. Their mechanism usually relies on a strong hydration layer, which acts as an energetic and physical barrier to proteins. In the chapter on nonfouling surfaces, the authors describe two main strategies for applying such systems: “graft-to-surface,” where the material adsorbs or binds from solution, and “graft-from-surface,” where polymer brushes grow from the surface. The first approach is technologically simpler; the second more easily achieves high packing density but usually requires more complex chemistry and substrate preparation.
In practice, this difference has engineering significance. If we merely want to quickly limit protein deposition on a relatively simple substrate, the simpler solution may suffice. However, if we require a durable, impermeable, and densely packed anti-adsorption layer, simply “sticking” molecules to the surface may not be enough. The book clearly emphasizes that the choice of method determines the packing density, the number of defects, and the durability of the final surface. This means that coatings are not evaluated solely based on their declared chemistry, but on whether they actually form a homogeneous, stable interface under operating conditions.
The third approach involves creating patterns, textures, and topographies. Here, the primary focus is not on changing the chemical composition, but on altering the geometry of what the cell or protein “sees.” The source emphasizes that surface topography influences cell adhesion, proliferation, migration, differentiation, and gene expression. Cells respond to both micro- and nanoscale features, not just the mere presence of the material. In the studies cited in the book, varying heights, sizes, and spacings of topographic structures altered the degree of mineralization, cell orientation, cell adhesion, and differentiation. This means that texture is not a mere ornament or a side effect of processing, but an active tool for controlling biological responses.
This is particularly evident in bone and dental implants. The book describes how an appropriately rough or three-dimensional surface layer can accelerate the early stages of healing, promote fibrin deposition, integrin binding, and micromechanical interlocking with bone. As a result, shear strength at the implant–bone interface increases, and load transfer improves. This is a good example of how texturing is not “blind improvement,” but an attempt to control a specific interfacial mechanism. However, caution is needed, as the same roughness that aids osseointegration may, in another application, increase the risk of bacterial colonization or hinder surface control.
Common mistakes, pitfalls, and false leads
The most common mistake is equating “better material” with “better biological response.” It’s too simplistic. Strength, fatigue resistance, and chemical stability do not yet explain what will happen at the tissue interface. In biomaterials, you can have an excellent structural material and a poor biological interface. You can also face the opposite problem: a highly biologically active surface mounted on a substrate that does not meet mechanical requirements. This is precisely why the premise that the material provides the implant with strength, while the surface determines the body’s response, is useful in design. It forces us to separate two questions that are often lumped together in classical engineering.
The second pitfall is the belief that a single surface property will solve the entire problem. In practice, there is no universal “biocompatibility setting.” Increasing hydrophilicity may limit the adsorption of certain proteins, but it does not necessarily improve tissue integration. Increasing roughness may promote the osteoblast response, but it may not be beneficial for an environment at risk of infection. The book itself notes that it is not yet known which parameter is most important for each specific biological response, so variables must be measured and correlated independently. This is a very important methodological guideline: instead of searching for a single magic number, one must build a map of relationships between several interface properties and a specific clinical goal.
The third pitfall concerns the thickness of the modification. The authors of the chapter on physicochemical modifications emphasize that modifications should be as thin as possible. Ideally, altering just the outermost few molecular layers – on the order of a few nanometers – would suffice, though in practice the layers must sometimes be thicker to ensure uniformity and durability. A coating that is too thick can alter the mechanical and functional properties of the device, as well as increase the risk of cracking and delamination. This is particularly important where the implant is subject to fatigue or friction. A layer that looks promising from a biological standpoint but mechanically peels off after some time does not solve the problem; it merely creates a new one.
The fourth misconception is treating the surface as a static state. The source demonstrates that some materials can reverse their surface organization upon transition from air to an aqueous environment. A surface measured “in dry conditions” may not be the same surface that proteins and cells encounter in the body. This has direct implications for research. If surface analysis does not account for the operating environment, one might optimize a parameter that ceases to have the same value or significance after implantation.
When a more advanced theory is needed
An advanced approach becomes necessary when intuitive terms like “smoother,” “more hydrophilic,” or “rougher” are no longer sufficient. Non-fouling surfaces are an example. Their function does not simply result from the fact that they are slippery, but from the fact that they form a stable hydration layer, the removal of which is energetically unfavorable for adsorbing proteins. The book demonstrates that PEG-based hydrophilic materials bind water through hydrogen bonds, while zwitterionic materials can do so even more strongly through electrostatically induced hydration. At this level, one must consider not only functional chemistry but also chain packing density, conformational freedom, and the stability of the layer’s anchoring.
Advanced theory is also needed when the surface is not only meant to be non-interfering but to actively guide cell behavior. In such cases, what matters is micro- and nanoscale geometry, local mechanics, the size, height, and spacing of topographic features, and sometimes even the orderliness or disorder of the pattern. This is precisely why research today employs topographic matrices and more systematic surface screenings. This is not about the academic complication of the subject, but about the fact that cells truly distinguish between scales and patterns of features, and the biological response ceases to be a linear function of a single parameter.
Why is the surface of an implant so important? – summary
In biomaterials, the success of an implant is often determined not by the bulk material itself, but by the surface it presents to the body. It is the surface that is the first point of contact with proteins, cells, and body fluids, and thus largely controls biocompatibility. For this reason, sensible implant design involves separating functions: the volume is intended to ensure mechanical properties and durability, while the surface is intended to elicit the appropriate biological response. This is the basis for the entire logic of modifying the surface without changing the entire material. One can remodel the existing outer layer, apply a new coating, or design a pattern and topography that will influence protein adsorption, cell behavior, tissue integration, or resistance to fouling. There is one condition: the modification must be truly interfacial, thin, durable, and tailored to a specific clinical goal. This is precisely why, in biomaterials, the surface is not a finishing detail, but one of the main tools in implant design.